Back pain is the most common complaint we treat. More than 80 percent of Americans experience back pain at some point in their lifetime. For many, the effect of back pain is an everyday battle which immensely impacts the quality of life. The pain we feel — whether in the back, the hip(s), or down the leg(s) — is the body’s request for change.
Back pain is not an indication something is broken, needing to be “fixed.” By taking the time to understand the problem and how it behaves, we can apply the right tool for the job — only then can we achieve a solution.
WHAT IT IS
Back pain is most commonly of mechanical nature, meaning how we move and use our body. If your back pain changes — for better or worse — with varying movement and positions accompanied by stiffness or loss of normal motion, you likely suffer from mechanical back pain.
The more common acute back pain is an episode lasting no longer than six weeks. Back pain is considered chronic when lasting greater than three months.
Because the nerve supply to your legs stems from the spinal cord within the spine, poor spinal mechanics can alter the signals from your brain to the muscles. It is not uncommon to experience symptoms such as pain, muscle weakness, or numbness and tingling anywhere down your leg(s), with or without local back symptoms!
WHAT BACK PAIN ISN'T
The pain we feel is simply a request from our brain to change. Pain is usually unassociated with damage, rather it’s an alert we need to change our physical behavior or else serious problem may result.
Mechanical back pain does not have to be debilitating and just because you have back pain does not mean you’re broken, needing to be “fixed”.
Just because you have pain doesn’t mean you need an MRI; just because your MRI shows “degeneration,” “disc bulges,” or “arthritis,” doesn’t mean it’s causing your pain. Back pain is often unassociated with the aforementioned structural changes commonly found from imaging, e.g. X-ray, CT scan, MRI. Furthermore, there’s a high prevalence of interpretive errors between radiologists. So, not only does imaging your spine result in a high rate of unrelated findings, the professionals interpreting them cannot concisely agree upon diagnoses!
In quality non-surgical care, it's important to minimize variables and rule out the spine as the pain generator.
Many medical diagnoses need to be thoroughly examined so that we don't "chase pain" and can understand WHY you're dealing with discomfort:
Sacroiliitis

The sacroiliac joint (SIJ) is the load-bearing, shock-absorbing union between the spine and pelvis. It is a mechanical link that connects the chain of locomotion to the rest of the body. This irregular, synovial and fibrocartilaginous joint is surrounded by a strong ligamentous-reinforced capsule and is minimally mobile (1,2).
More
Piriformis Syndrome

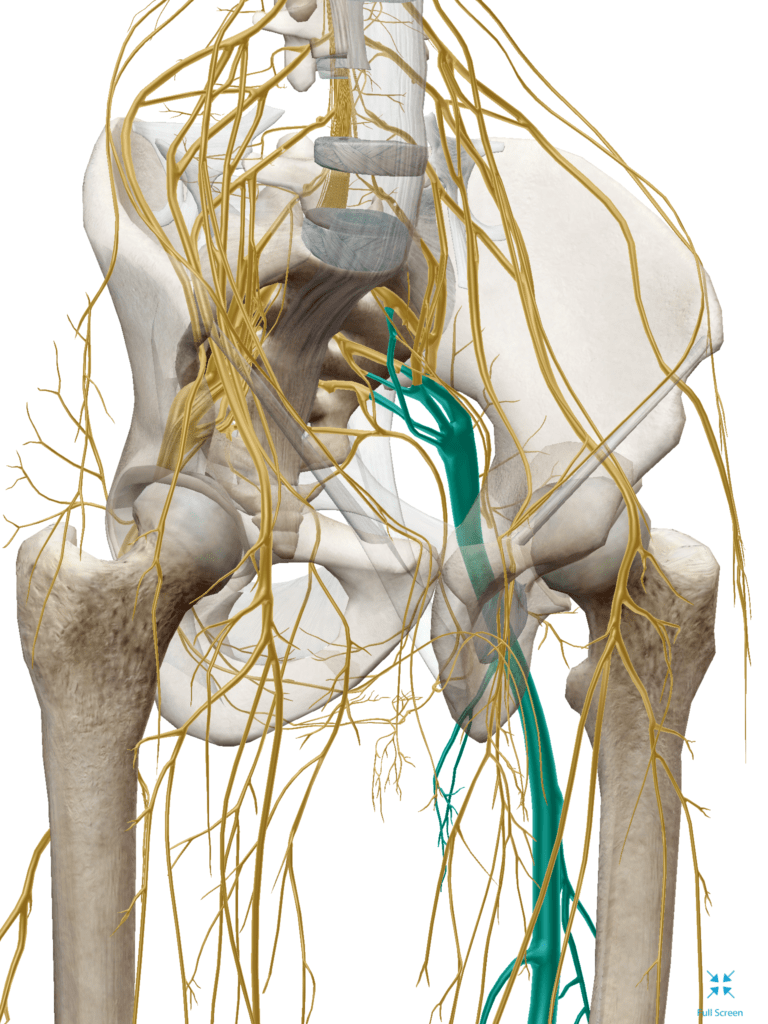
Piriformis syndrome arises when a irritated piriformis muscle compresses the sciatic nerve (1). This pressure causes ischemia, congestion, local inflammation and radicular complaints (2). Researchers estimate that piriformis syndrome contributes to up to one third of all back pain (3,4).
The piriformis muscle originates on the anterolateral surface of the mid-portion of the sacrum and inserts on the superior medial aspect of the greater trochanter. When the hip is extended, the piriformis functions primarily as an external rotator of the thigh, with secondary contributions toward flexion. The muscle assists in abduction when the hip is flexed to 90 degrees. (3) The sciatic nerve has a variable relationship to the piriformis muscle. In the majority of the population, the sciatic nerve travels deep to the muscle. Approximately one fourth of the population is anatomically predisposed to piriformis syndrome because their sciatic nerve passes through the muscle, splits the muscle or both. (5,6) Symptoms of piriformis syndrome may begin abruptly as the result of a traumatic event, or may develop slowly in response to repeated irritation. Piriformis muscle irritation and hypertonicity can result from a strain, a fall onto the buttocks or catching oneself from a “near fall”. In other instances, the process may begin following repetitive microtrauma, like long distance walking, stair climbing or from chronic compression- i.e.sitting on the edge of a hard surface or a wallet. (8,9) Presenting complaints for piriformis syndrome include pain, paresthesia or numbness beginning in the gluteal region and radiating along the course of the sciatic nerve. Additional symptoms may develop from local trigger point referral into the proximal thigh, sacroiliac and hip regions. (9) Symptoms are often provoked by holding any one position for longer than 15-20 minutes- particularly prolonged sitting or standing. Positional changes may provide transient relief. Patients may report increasing discomfort when walking, running, stair climbing, riding in a car or arising from a seated position. Activities that involve hip internal rotation, like sitting cross-legged, may exacerbate symptoms (10).Piriformis syndrome shares several common characteristics and may even co-exist with other lumbopelvic problems. The differential diagnosis for piriformis syndrome includes; hip pathology, fracture, lumbar compression fracture, discitis, trochanteric bursitis, sacroiliitis, sacroiliac joint dysfunction, lumbar radiculopathy, spinal stenosis and viscerosomatic referred pain.
References 1. Yeoman W. The relation of arthritis of the sacroiliac joint to sciatica. Lancet. 1928;ii:1119-22.2. Williams PL, Warwick R. Gray's Anatomy. 36th ed. Philadelphia, Pa: WB Saunders Co; 1980.3. Papadopoulos EC, Khan SN. Piriformis syndrome and low back pain: a new classification and review of the literature. Orthop Clin North Am. 2004;35:65-71.4. Pace JB, Nagle D. Piriformis syndrome. West J Med. 1976;124:435-439.5. Beason LE, Anson B.J. The relation of the sciatic nerve and its subdivisions to the piriformis muscle. Anat Record. 1937;70:1-5.6. Pecina M. Contribution to the etiological explanation of the piriformis syndrome. Acta Anat (Basel). 1979;105:181-187.7. http://physioplus.blogspot.com/2008/09/piriformis-syndrome.html, retrieved 10/138. Foster MR. Piriformis syndrome. Orthopedics. 2002;25:821-8259. Travell J, Simons D. Myofascial Pain and Dysfunction, Vol 2. Williams and Wilkins 1992. pp 186-21410. Magee DJ. Orthopedic Physical Assessment. 3rd ed. Philadelphia, Pa: WB Saunders Co; 1997.
IT Band Syndrome
Iliotibial band syndrome (aka Iliotibial Band Friction Syndrome) describes an irritation of the tissues near the distal attachment of the iliotibial band. This overuse syndrome is particularly common in runners and cyclists. (1-3)
Iliotibial band syndrome (aka Iliotibial Band Friction Syndrome) describes an irritation of the tissues near the distal attachment of the iliotibial band. This overuse syndrome is particularly common in runners and cyclists. (1-3) The ITB is divided anatomically into two distinct portions- a proximal “tendinous” segment and a distal “ligamentous” component. (4) The proximal portion begins as a sheath encasing the tensor fascia lata muscle. This sheath anchors the tensor fascia lata to the iliac crest and also receives the majority of the gluteus maximus tendon. (5) The dense fibrous ITB then courses distally with a deep component that attaches to the femoral shaft via the strong lateral intermuscular septum and linea aspera. (4) Distally, the tendinous portion “fans” before terminating near the lateral epicondyle. (4) The ITB then transitions to its ligamentous component, spanning from the lateral epicondyle of the femur to Gerdy’s tubercle on the anterolateral aspect of the tibia. (5)The iliotibial band is a conduit for forces generated by the TFL and gluteus maximus (i.e. thigh abduction, flexion, extension, and external rotation). The deep fascial component, which attaches to nearly the entire length of the femur, is most taut when the gluteus maximus and TFL contract. This “tensile” action significantly increases during single leg stance and serves to counteract medial bowing of the femur, while lateral bowing is minimized by “compression”. (4,6)ITB syndrome is common in populations exposed to repetitive knee flexion and extension while in a single leg stance. (9) The problem is particularly prevalent in runners, where it comprises almost ¼ of all lower extremity injuries. (2,3,10-17) Ultimately, ITB syndrome affects up to 12% of all runners. (10) The condition is also frequently seen in cycling, weight lifting, skiing, soccer, basketball, field hockey, and competitive rowing. The typical presentation for ITB syndrome is a runner or cyclist complaining of “sharp” or “burning” pain approximately 2 cm above on the outside of the knee – near the lateral femoral condyle. (9) Pain may radiate slightly above or below. (9) Symptoms are provoked by activities that require repetitive knee flexion and extension. Symptoms are more likely as activities proceed. (9) Less severe presentations may report pain only during activity, but as the condition progresses, symptoms become more persistent. References1. S. P. Messier, D. G. Edwards, D. F. Martin et al., “Etiology of iliotibial band friction syndrome in distance runners,” Medicine and Science in Sports and Exercise, vol. 27, no. 7, pp. 951–960, 1995.2. Ellis R, Hing W, Reid D. Iliotibial band friction syndrome–a systematic review. Man Ther. Aug 2007;12(3):200-8.3. Hamill J, Miller R, Noehren B, Davis I. A prospective study of iliotibial band strain in runners. Clin Biomech (Bristol, Avon). Jun 24 20084. Fairclough J, Hayashi K, Toumi H, et al. The functional anatomy of the iliotibial band during flexion and extension of the knee: implications for understanding iliotibial band syndrome. J Anat, 2006;208:309-316.5. Standring S. Gray's Anatomy: the Anatomical Basis of Clinical Practice. 39. Edinburgh: Elsevier/Churchill Livingstone; 2004.6. Michaud T. The Real Cause of Iliotibial Band Syndrome Dynamic Chiropractic November 18, 2012, Vol. 30, Issue 24Fetto J, Leali A, Moroz A Evolution of the Koch model of the biomechanics of the hip: clinical perspective. J Orthop Sci. 2002; 7(6):724-30.7. Drogset JO, Rossvoll I, Grøntvedt T Surgical treatment of iliotibial band friction syndrome. A retrospective study of 45 patients. Scand J Med Sci Sports. 1999 Oct; 9(5):296-8.8. Fetto J, Leali A, Moroz A Evolution of the Koch model of the biomechanics of the hip: clinical perspective. J Orthop Sci. 2002; 7(6):724-30.9. M. Fredericson and A. Weir, “Practical management of iliotibial band friction syndrome in runners,” Clinical Journal of Sport Medicine, vol. 16, no. 3, pp. 261–268, 200610. Linenger JMCC. Is iliotibial band syndrome overlooked? Phys Sports Med. 1992;20:98–108.
Sciatica Treatment
Sciatica is not a true medical diagnosis but rather a symptom of an underlying medical condition. There are a few common lower back problems that can cause sciatica symptoms. These include a radiculopathy, bulging disc, degenerative disc disease, spondylolisthesis, or spinal stenosis
Sciatica is often characterized by one or more of the following symptoms: constant pain in one side of the buttock or leg (rarely in both legs), pain that is worse when sitting, leg pain that is often described as burning or tingling, weakness or numbness, sharp pain that may make it difficult to stand up or walk, and pain that radiates down the leg and possibly into the foot and toes.
We typically find sciatica symptoms aren’t always as black and white as it’s drawn up in the books. The patient typically can’t draw a straight line with a pen from the back straight down the leg. Rather, the symptoms are variable and change based on positions and movements. The patient may sometimes have pain the glute, their hamstrings feel “different”, and they have an odd sensation in the calf. Sciatic pain can vary from intermittent and irritating to constant and debilitating.
Symptoms are usually based on the location of the pinched nerve. The sciatic nerve is the largest single nerve in the body and is made up of individual nerve roots that start by branching out from the spine in the lower back and then combine to form the "sciatic nerve." Sciatica symptoms occur when the large sciatic nerve is irritated or compressed at or near its point of origin around the lower back. The sciatic nerve starts in the low back, typically at the third lumbar segment. At each level of the lower spine, a nerve root exits from the inside of the spinal canal, and each of these respective nerve roots then come together to form the large sciatic nerve.
The sciatic nerve runs from the lower back, through the buttock, and down the back of each leg. Portions of the sciatic nerve then branch out in each leg to innervate certain parts of the leg—the thigh, calf, foot, and toes. The specific sciatica symptoms—the leg pain, numbness, tingling, weakness, and possibly symptoms radiating into the foot—largely depend on where the nerve is pinched.
Often, a particular event or injury does not cause sciatica— the most common cause of sciatica is “for no apparent reason” – it tends to develop over time. Our chiropractor in Plymouth helps you understand your sciatica symptoms and will quickly find you a solution or get you to the provider who can help.
More info on: Sciatica Treatment
COMMON CAUSES OF BACK PAIN
Mechanical back pain is most commonly caused by poor body mechanics and postural habits.
Humans are meant to move and move often — not sit in chairs and stare at electronic screens for hours on end. From infancy through the first year of life, we learn to how to move, setting us up for the rest of our lives.
Mechanical back pain can occur suddenly from something as simple as bending over to put on your socks, or can gradually occur for no apparent reason.
Pain from bending over is not because forward bending is inherently bad, rather it’s the result of the accumulated stress of repetitive bending — the straw that broke the camel's back, so to say.
Think about the average desk worker’s day: sit for breakfast, sit in the car to work, sit at the desk, sit for lunch, back to sitting at the desk, sit in the car back home, sit in front of the T.V. — you get the point.
The accumulative postural stress of sitting as a daily habit is like bending your finger backward. It may not hurt at first, but the longer you hold it there, and the more pressure you apply over time, it will start to feel uncomfortable and aching. When you let go of the finger, you’ll have a residual ache, but you’ll notice the pain quickly subsides. This is mechanical pain, and is similar to what the typical American with back pain experiences.
So, what happens after you lift something heavy with poor form after sitting all day? It’s like cranking that finger back as far as it can go…and it’s probably going to hurt long after you let go of it!
COMMON TREATMENTS FOR BACK PAIN
The most common treatments are rest, medication, physical therapy, chiropractic, acupuncture, massage, and other various conservative therapies.
While most acute bouts of back pain will resolve on their own within a few weeks, the risk of recurrence is very high. The greatest risk of injury is a previous injury.
Few individuals need surgery for back pain. Have a disc bulge? Even if it’s relevant, lumbar disc herniations have been shown to resolve on their own without surgery.
If you have intense and unrelenting radiating pain down the leg with progressive muscle weakness, bladder or bowel symptoms, or specific structural problems not responding to conservative therapy, surgery may be warranted.
WHAT YOU CAN DO ABOUT BACK PAIN
With all mechanical pain, there’s a ‘what’ and a ‘why’ — what the problem is and why it’s occurring in the first place. To achieve resolution it’s crucial to not only identify and correct the problem at hand but address the behaviors which lead to the issue.
Our approach isn’t to just “fix” the problem, rather understand what it is and what it isn’t, so the correct treatment is applied to the right problem — only then can we solve the problem. Why use a hammer if you’re not positive it’s a nail? The last thing you want is to hammer away at a screw!
REACH initiates treatment for back pain by utilizing the Mckenzie Method (MDT). MDT is a proven system of examination, treatment, and classification of spinal, joint, and other musculoskeletal pain, backed by years of research, evidence, and practice. The System has been shown to be low cost, fast, and effective even for chronic pain.
By exploring simple movements in repetition that improve or worsen your symptoms and functional baselines (i.e. walking, stepping, lifting, reaching, bending, muscle strength), we can understand how your pain behaves.
If a mechanical force caused the problem then it is logical that a mechanical force may be part of the solution. The MDT system is designed to identify the mechanical problem and develop a plan to correct or improve the mechanics, thus decrease or eliminate the pain and functional problems. Further, the system tells us what treatment tool to use at the appropriate time, eliminating the guessing game.
Once we identify a movement(s) that improves your baselines, you’re on your way to controlling your pain yourself, not needing your holistic chiropractor on a repetitive basis. If your problem is something we are unable to treat, the McKenzie assessment will tell us this within the first few visits, and then we recommend the next best course of action to find you a solution.
5.0★ rated by 450+ patients across Plymouth and metro Detroit.